
Guide to Hepatorenal Syndrome Severe Liver Complication
Learn about Hepatorenal Syndrome (HRS), a severe complication of advanced liver disease. This guide covers symptoms, causes, diagnosis, and treatment options for this life-threatening condition.


Introduction
Hepatorenal syndrome (HRS) is a life-threatening and severe liver complication that represents a critical turning point in advanced liver disease. It is a unique type of kidney failure that occurs because the liver is failing, not due to direct damage to the kidneys themselves. This paradox makes it one of the most challenging complications of cirrhosis. Understanding hepatorenal syndrome is crucial for patients and caregivers, as early recognition can significantly impact outcomes. This guide will demystify HRS, explaining its causes, symptoms, and the complex connection between your liver and kidneys. We will walk you through the latest diagnostic criteria, explore cutting edge and standard treatment options, including the role of liver transplantation, and discuss what the prognosis truly means. Our goal is to equip you with the knowledge to have informed conversations with your healthcare team.
H2: What is Hepatorenal Syndrome? The LiverKidney Connection
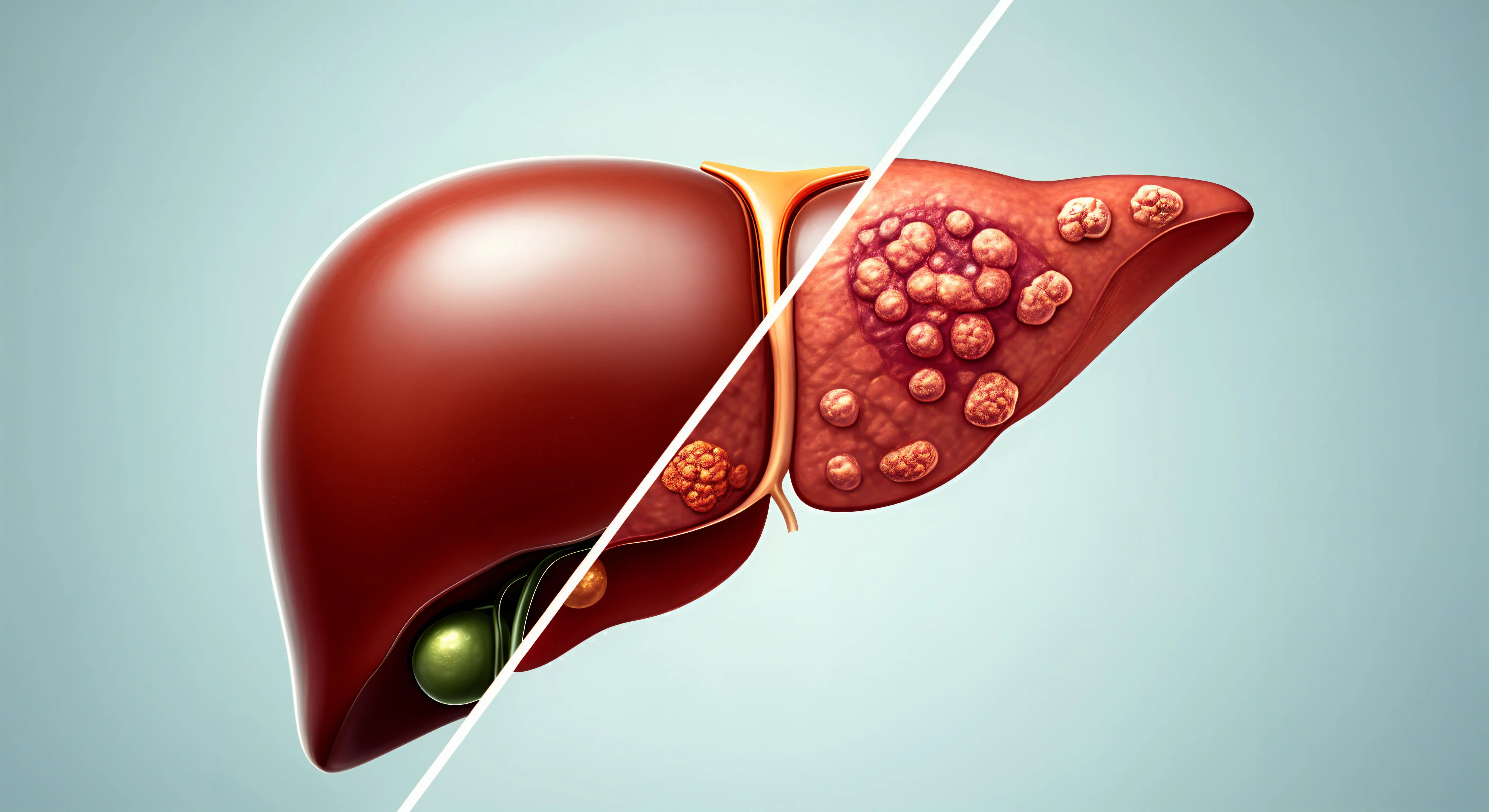
Hepatorenal syndrome is a functional, progressive kidney failure that develops in individuals with advanced liver disease, most commonly cirrhosis and acute liver failure. The key thing to understand is that the kidneys themselves are often structurally normal. The problem lies in profound abnormalities in blood flow. When the liver becomes severely scarred, it causes blood pressure changes throughout the body, leading to intense narrowing of the blood vessels that supply the kidneys. This drastically reduces blood flow, causing the kidneys to stop filtering toxins and producing urine effectively. It's a vicious cycle where the sick liver creates an environment that is toxic to the kidneys.
H3: The Two Main Types: HRS1 and HRS2
Medical professionals classify hepatorenal syndrome into two distinct types, which have important implications for treatment and prognosis:
- Type 1 (HRS1): This is a rapidly progressive form. It is defined by a doubling of the serum creatinine level to greater than 2.5 mg/dL in less than two weeks. HRS1 is a medical emergency with a very poor short-term prognosis without swift intervention. It often follows a triggering event like a spontaneous bacterial peritonitis (SBP) infection, acute alcoholic hepatitis, or a major gastrointestinal bleed.
- Type 2 (HRS2): This type develops more slowly and is characterized by a steady, moderate reduction in kidney function (serum creatinine levels typically between 1.5 and 2.5 mg/dL). The primary clinical problem in HRS2 is stubborn, diuretic-resistant ascites (fluid buildup in the abdomen) that is difficult to manage. While the progression is slower, it still signifies a serious worsening of the underlying liver disease.
H2: What Causes Hepatorenal Syndrome? The Underlying Mechanism
The development of HRS is a complex process, but it primarily stems from advanced cirrhosis and portal hypertension.
H3: The Role of Portal Hypertension and Vasodilation
In a cirrhotic liver, scar tissue blocks normal blood flow, causing pressure to build up in the portal vein—a condition known as portal hypertension. This high pressure forces blood into smaller blood vessels in the abdomen (splanchnic circulation), causing them to dilate or widen significantly. This massive vasodilation pools blood in the abdomen, effectively reducing the volume of blood circulating effectively to the rest of the body.
H3: How a Sick Liver Tricks the Kidneys into Failing
The body misinterprets this reduced effective blood volume as being due to blood loss or dehydration. It activates powerful compensatory mechanisms to conserve volume and raise blood pressure:
- The reninangiotensinaldosterone system (RAAS) is activated.
- The sympathetic nervous system goes into overdrive.
- The body releases antidiuretic hormone (ADH).
These systems cause intense constriction of blood vessels in the kidneys and throughout the body. Unfortunately, while this might temporarily help circulation elsewhere, it catastrophically reduces blood flow to the kidneys themselves. The kidneys, starved of blood, begin to fail. This explains why giving IV fluids alone doesn't work; the problem isn't a lack of fluid volume but a massive misdistribution of blood flow.
H2: Recognizing the Signs: Symptoms of Hepatorenal Syndrome
The symptoms of hepatorenal syndrome are often a combination of worsening liver failure and new onset kidney failure. It can be difficult to distinguish them from the symptoms of advanced cirrhosis itself.
H3: Symptoms from Worsening Liver Disease
- Yellowing of the skin and eyes (jaundice)
- Increased abdominal girth and pain from ascites
- Confusion, drowsiness, and slurred speech (hepatic encephalopathy)
- Tendency to bleed or bruise easily
H3: Symptoms from Emerging Kidney Failure
- Markedly reduced urine output: This is a hallmark sign.
- Fatigue, weakness, and nausea
- Swelling in the legs, feet, or ankles (edema)
- In later stages, shortness of breath due to fluid buildup in the lungs
If you have known liver disease and notice a significant decrease in how often you urinate, or any of these symptoms, it is a critical warning sign. Consult a doctor online with Apollo24|7 for immediate evaluation to determine the next steps.
H2: How is Hepatorenal Syndrome Diagnosed?
Diagnosis requires careful evaluation, as there is no single test for HRS. Doctors use a set of strict criteria to rule out other causes of kidney failure.
H3: The International Club of Ascites (ICA) Criteria
The diagnosis is based on the ICA criteria, which include:
- Presence of cirrhosis with ascites.
- A rise in serum creatinine level (>1.5 mg/dL).
- No improvement in kidney function after at least 48 hours of stopping diuretics and receiving albumin infusion.
- Absence of shock.
- No current or recent use of nephrotoxic drugs.
- No signs of structural kidney injury (e.g., no proteinuria, no abnormal findings on ultrasound).
H3: Essential Tests and Procedures
To meet these criteria, your doctor will order several tests:
- Blood Tests: To measure creatinine, electrolytes, liver enzymes (AST, ALT), bilirubin, and albumin. Apollo24|7 offers convenient home collection for these crucial tests, allowing for easier monitoring.
- Urine Tests: To check sodium and protein levels.
- Ultrasound: To examine the kidneys and liver and rule out obstruction.
H2: Treatment Options for Hepatorenal Syndrome
The goals of treatment are to improve kidney function, prolong survival, and serve as a bridge to liver transplantation.
H3: FirstLine Pharmacological Therapy: Vasoconstrictors and Albumin
The cornerstone of hepatorenal syndrome treatment is the use of vasoconstrictor drugs paired with intravenous albumin. The drugs (e.g., terlipressin, noradrenaline, midodrine + octreotide) counteract the splanchnic vasodilation, squeezing the dilated blood vessels in the abdomen and improving blood flow to the kidneys. Albumin helps expand the plasma volume and improves the effectiveness of the vasoconstrictors.
H3: Bridge Therapies: TIPS and Renal Replacement Therapy
- Transjugular Intrahepatic Portosystemic Shunt (TIPS): A procedure where a radiologist places a stent to create a bypass between the high-pressure portal vein and a lowpressure hepatic vein. This reduces portal pressure and can improve kidney function in selected patients.
- Renal Replacement Therapy (Dialysis): Used for patients with severe kidney failure who are not responding to drugs, primarily as a bridge to transplant to manage toxins and fluid overload.
H3: The Only Definitive Cure: Liver Transplantation
For eligible patients, liver transplantation is the only treatment that addresses the root cause of HRS. It offers the best chance for long-term survival and recovery of kidney function. Posttransplant, kidney function often recovers, though some patients may require a combined liver/kidney transplant.
H2: Prognosis and Life Expectancy with HRS
The prognosis for hepatorenal syndrome has historically been very poor. Without treatment, the median survival for Type 1 HRS is less than two weeks. With modern pharmacological treatment, survival rates at three months can improve to 4050%. For Type 2 HRS, the median survival is about 6 months. These numbers underscore the critical importance of early detection and aggressive treatment. Successfully bridging to a liver transplant dramatically improves long-term survival outcomes.
H2: Can Hepatorenal Syndrome Be Prevented?
While not always preventable, the risk can be reduced in patients with advanced cirrhosis through:
- Prompt treatment of infections (like SBP) with antibiotics and albumin.
- Avoiding nephrotoxic drugs (e.g., NSAIDs like ibuprofen).
- Careful use of diuretics under a doctor's supervision.
- Avoiding largevolume paracentesis (draining ascites fluid) without albumin infusion.
- Managing the underlying liver disease by abstaining from alcohol and following a prescribed diet.
H2: When to Seek Immediate Medical Attention
If you have cirrhosis and experience any of the following, seek emergency care:
- A rapid, significant decrease in urine output.
- Rapid worsening of confusion or drowsiness.
- Severe abdominal pain or rapid enlargement of the abdomen.
- Fever, which could indicate an infection.
- Vomiting blood or passing black, tarry stools.
Custom Image Concepts
1. Image 1: The HRS Pathway Diagram
- Concept: A flow chart showing the progression from Liver Cirrhosis > Portal Hypertension > Splanchnic Vasodilation > Reduced Effective Blood Volume > Compensatory Vasoconstriction > Renal Vasoconstriction > Kidney Failure (HRS).
- Alt Text: Diagram explaining the pathophysiology and cause of hepatorenal syndrome in liver cirrhosis.
2. Image 2: HRS1 vs. HRS2 Comparison Infographic
- Concept: A side by side comparison table in visual form. One side shows a fast-moving clock and a steeply climbing creatinine chart for HRS1. The other shows a slowmoving clock and a gradually climbing chart for HRS2, with icons for refractory ascites.
- Alt Text: Infographic comparing the differences between Type 1 and Type 2 hepatorenal syndrome.
3. Image 3: Treatment Modalities
- Concept: Icons representing different treatments: a syringe for vasoconstrictors, an IV bag for albumin, a diagram of a TIPS procedure, and a donor liver icon for transplantation.
- Alt Text: Visual guide to the various treatment options available for hepatorenal syndrome.
Quick Takeaways: Key Points on HRS
- Hepatorenal Syndrome (HRS) is a functional kidney failure caused by advanced liver disease.
- There are two types: HRS1 (fast and severe) and HRS2 (slower with diuretic-resistant ascites).
- The root cause is portal hypertension leading to reduced blood flow to the kidneys.
- A key symptom is a significant reduction in urine output in someone with known cirrhosis.
- Diagnosis follows strict international criteria to rule out other kidney problems.
- Treatment involves vasoconstrictor drugs + albumin, with liver transplant being the only cure.
- The prognosis is serious but has improved with modern treatment, especially for those who receive a transplant.
- Immediate medical attention is required if symptoms appear.
Conclusion
Hepatorenal syndrome is a daunting complication of endstage liver disease, but it is not an insurmountable one. Understanding the intimate link between your liver and kidneys is the first step toward recognizing the warning signs. While the diagnosis is serious, medical advancements have provided crucial tools to manage it. Treatments like terlipressin and albumin can reverse kidney failure in a significant number of patients, acting as a vital bridge to the only definitive solution: liver transplantation. The key to navigating this challenging condition lies in vigilant monitoring, close collaboration with a specialized healthcare team, and seeking immediate care at the first sign of trouble. If you or a loved one is living with advanced liver disease, having a clear action plan and understanding HRS can make a profound difference in outcomes and quality of life.
Consult a General Physician
Consult a General Physician

Dr. Rajib Ghose
General Physician/ Internal Medicine Specialist
25 Years • MBBS
East Midnapore
VIVEKANANDA SEBA SADAN, East Midnapore

Dr. Impana G N
Physician/ Internal Medicine/ Covid Consult
11 Years • MBBS,DNB FAMILY MEDICINE, MNAMS ,CCEBDM
Mysuru
Apollo BGS Hospital Adichuchanagiri Road, Mysuru

Dr. Ajay K Sinha
General Physician/ Internal Medicine Specialist
30 Years • MD, Internal Medicine
Delhi
Apollo Hospitals Indraprastha, Delhi
(225+ Patients)

Dr. Sougata Kumar
General Practitioner
9 Years • MBBS
East Midnapore
VIVEKANANDA SEBA SADAN, East Midnapore

Dr. Vivek D
General Physician
4 Years • MBBS
Bengaluru
PRESTIGE SHANTHINIKETAN - SOCIETY CLINIC, Bengaluru
Consult a General Physician for the best advice
Dr. Rajib Ghose
General Physician/ Internal Medicine Specialist
25 Years • MBBS
East Midnapore
VIVEKANANDA SEBA SADAN, East Midnapore
Dr. Impana G N
Physician/ Internal Medicine/ Covid Consult
11 Years • MBBS,DNB FAMILY MEDICINE, MNAMS ,CCEBDM
Mysuru
Apollo BGS Hospital Adichuchanagiri Road, Mysuru
Dr. Ajay K Sinha
General Physician/ Internal Medicine Specialist
30 Years • MD, Internal Medicine
Delhi
Apollo Hospitals Indraprastha, Delhi
(225+ Patients)
Dr. Sougata Kumar
General Practitioner
9 Years • MBBS
East Midnapore
VIVEKANANDA SEBA SADAN, East Midnapore
Dr. Vivek D
General Physician
4 Years • MBBS
Bengaluru
PRESTIGE SHANTHINIKETAN - SOCIETY CLINIC, Bengaluru
More articles from Liver disease


Frequently Asked Questions
1. Is hepatorenal syndrome reversible?
Yes, hepatorenal syndrome can be reversed with pharmacological treatment using vasoconstrictors and albumin in a significant proportion of patients. However, the reversal is often temporary unless the underlying liver disease is treated. The only permanent reversal comes from a successful liver transplant.
2. What is the difference between HRS and other kidney failure?
The key difference is that in HRS, the kidneys are structurally normal but are not functioning due to poor blood flow caused by liver failure. In other types of kidney failure (e.g., from diabetes or hypertension), the kidney tissue itself is directly damaged.
3. How long can you live with hepatorenal syndrome without a transplant?
Life expectancy without treatment is very short, especially for Type 1 HRS (less than two weeks). With treatment, survival can be extended to several months, but the long-term prognosis without a liver transplant remains poor due to the severity of the underlying liver disease.
4. Can dialysis cure hepatorenal syndrome?
No, dialysis does not cure HRS. It is a supportive therapy that performs the job of the failed kidneys by filtering toxins and removing excess fluid from the blood. It is used as a temporary measure to keep a patient stable while awaiting transplant or to see if other medications will help the kidneys recover function.
5. What are the first signs of hepatorenal syndrome?
The most consistent early sign is a noticeable decrease in urine output. Other signs include worsening ascites that do not improve with diuretics, increased confusion (hepatic encephalopathy), and fatigue. Any sudden change in the condition of a person with cirrhosis should be evaluated immediately by a doctor.