
Guide to 8 Silent Signs Brain Tumor You Should Know
Don't ignore the subtle clues. Learn about the 8 silent signs of a brain tumor that are often missed. Early detection saves lives. Read our essential guide now.

Written by Dr. Dhankecha Mayank Dineshbhai
Reviewed by Dr. M L Ezhilarasan MBBS
Last updated on 13th Jan, 2026

Introduction
Most brain tumors don’t announce themselves with dramatic symptoms overnight. Instead, they can whisper—small, subtle changes that are easy to misread as stress, age, or “just one of those things.” In this guide, we’ll walk you through eight silent signs of a brain tumor that the general public often overlooks, why these signals happen, and how to tell when it’s time to get checked. You’ll learn how brain tumors cause symptoms depending on their location, which patterns matter, what else could explain similar symptoms, and the smart next steps to take. We’ll keep the science approachable and the advice practical, with examples, expert-backed insights, and simple tools you can use today. If symptoms persist beyond two weeks or escalate, consult a doctor online with Apollo 24|7 for further evaluation. Early attention doesn’t mean alarm—it means peace of mind. Let’s demystify the quiet side of brain tumor symptoms so you can act with confidence.
Why Subtle Brain Tumor Symptoms Are Easy to Miss?
The brain runs everything—movement, mood, memory, hormones, and senses—so symptom changes depend on where a tumor grows and how quickly it expands. Slow-growing tumors may “blend in” with daily life, causing mild, fluctuating symptoms that feel like stress, migraines, or aging. For example, a small tumor in the frontal lobe might nudge personality, concentration, or planning skills long before it causes pain. Pituitary tumors can quietly disrupt hormones, showing up as irregular periods, libido changes, or unexplained fatigue rather than headaches. And because the brain has no pain receptors, you won’t feel a tumor directly—symptoms often result from pressure on nearby tissues or increased pressure in the skull, which may only appear as morning headaches or nausea.
Competing causes add to the confusion: migraines, anxiety, sleep apnea, perimenopause, ear infections, and vitamin deficiencies can mimic many brain tumor signs. That’s why context matters: new, progressive, or pattern-changing symptoms—especially when clustered (like new headaches plus vision changes)—deserve attention. A helpful rule of thumb: if something about a symptom is new, worsening, or unlike your “usual,” note it and discuss it with a clinician. If symptoms persist beyond two weeks or escalate, consult a doctor online with Apollo 24|7 for further evaluation.
Consult a Top General Physician
How do Brain Tumors Cause Symptoms? (Location, Size, and Pressure)
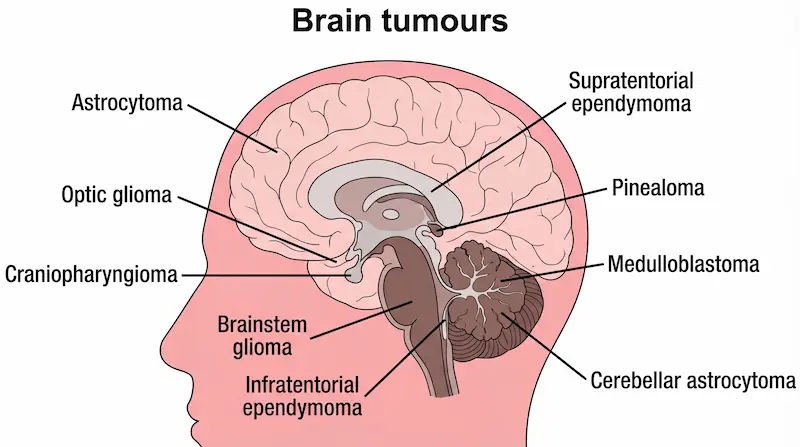
- Location: The brain is mapped like a city. Frontal lobes influence behavior and executive function; temporal lobes handle memory and language; occipital lobes manage vision; cerebellum coordinates balance; the brainstem controls essential functions like breathing and swallowing. A small lesion in the right spot can create specific deficits (e.g., word-finding trouble with left temporal lobe involvement).
- Size and growth rate: A small, fast-growing tumor can cause symptoms sooner than a larger, slow-growing one. Rapid growth causes edema (swelling), which amplifies pressure effects.
- Mass effect and intracranial pressure: When space is limited, pressure rises, leading to headaches that are worse in the
morning (when CO2 rises during sleep) and nausea/vomiting not explained by a stomach bug. - Irritation of cortex: Seizures often result when tumors irritate the brain’s electrical networks—even non-cancerous
(benign) tumors can cause seizures. - Hormonal disruption: Pituitary tumors alter hormones like prolactin, thyroid hormones, or cortisol, which can drive subtle systemic changes, such as menstrual irregularities or unexplained weight changes.
8 Silent Signs to Watch (And What They Can Mean)
1) New or Changing Headaches—Especially Morning or with Position
- What it looks like: Headaches that are new for you, steadily worsening over weeks, worse on waking, or triggered by coughing/straining/lying down. Sometimes accompanied by nausea or vomiting without GI illness.
- Why it happens: Changes in intracranial pressure and irritation of pain-sensitive structures (meninges, blood vessels).
- What raises concern: Headache plus early morning vomiting, any new neurological deficit (weakness, speech trouble), or headache that’s different from your usual migraine pattern.
- Action: Track timing, triggers, and severity for two weeks. If persistent or progressive, see a clinician. If you have a thunderclap headache (sudden, severe), seek emergency care.
2) Subtle Personality, Mood, or Cognitive Changes
- What it looks like: Irritability, apathy, impulsivity, reduced motivation, trouble focusing, planning, or multitasking.
Family or coworkers may notice before you do. - Why it happens: Frontal and temporal lobe involvement affects executive function and emotional regulation.
- What raises concern: Gradual change over weeks to months, interfering with work or relationships; memory lapses that aren’t typical for you.
- Action: Ask someone you trust if they’ve noticed changes. Document examples. Consider a cognitive screening visit if symptoms persist.
3) Unexplained Nausea or Vomiting (Especially with Headache)
- What it looks like: Morning nausea, vomiting without diarrhea or fever, motion sensitivity that’s new for you.
- Why it happens: Elevated intracranial pressure stimulates the vomiting center in the brainstem.
- What raises concern: Nausea paired with new headaches, vision changes, or dizziness.
- Action: Rule out GI causes first; if symptoms persist beyond 1–2 weeks or cluster with neuro signs, get evaluated.
4) Vision or Hearing Changes You Can’t Explain
- What it looks like: Blurred or double vision, loss of peripheral vision (bumping into things), transient visual shadows, new hearing loss in one ear, or persistent tinnitus.
- Why it happens: Tumors near the optic pathways, occipital lobe, brainstem, or cranial nerves (e.g., vestibular schwannomas).
- What raises concern: Progressive visual field loss, double vision, or one-sided hearing loss.
- Action: Eye exam (look for papilledema) and neuro evaluation. If needed, an MRI is the preferred imaging for brain
structures. Apollo 24|7 can arrange teleconsultation and guide the next steps.
5) New Onset Seizures in Adults
- What it looks like: Full-body convulsions or subtle focal seizures—sudden speech arrest, rhythmic twitching of one limb, déjà vu episodes, strange smells, brief confusion.
- Why it happens: Cortical irritation. Brain tumors are a leading cause of first-time seizures in adults without prior epilepsy.
- What raises concern: Any first-time seizure warrants urgent evaluation.
- Action: Seek emergency care. After stabilization, MRI is typically ordered. Learn basic seizure first aid: protect the head, don’t restrain, time the event, roll to the side, and call for help if it lasts >5 minutes.
6) Weakness, Numbness, or Clumsiness on One Side
- What it looks like: Dropping objects, foot drag, subtle facial droop, loss of fine motor skills, balance issues, or a new,
unexplained fall. - Why it happens: Motor cortex, cerebellum, or brainstem involvement.
- What raises concern: Progressive asymmetry, pairing with speech difficulty or visual changes.
- Action: Seek prompt assessment, especially if symptoms come on quickly or evolve over days to weeks.
7) Speech, Language, or Understanding Difficulties
- What it looks like: Word-finding trouble, mixing words, difficulty understanding fast speech, or writing that becomes disorganized.
- Why it happens: Left temporal or frontal lobe (language areas) involvement.
- What raises concern: This is new for you and not explained by fatigue or anxiety.
- Action: Note specific examples and frequency. Evaluation may include a neuro exam and imaging.
8) Hormonal or Menstrual Changes (Pituitary Clues)
- What it looks like: Irregular periods, milk discharge (galactorrhea), low libido, erectile dysfunction, unexplained weight change, heat/cold intolerance.
- Why it happens: Pituitary tumors alter hormone production, often without pain.
- What raises concern: Persistent endocrine changes without another explanation.
- Action: Discuss hormonal testing (e.g., prolactin, thyroid function). Apollo 24|7 offers convenient home collections for labs like TSH, prolactin, cortisol, and HbA1c when indicated.
When to Worry?: Red Flags, Timelines, and Next Steps
Red flags that warrant prompt medical evaluation:
- New, progressive headaches lasting longer than two weeks, especially morning-worse or positional, or with vomiting.
- Any new adult-onset seizure.
- Focal neurological deficits: weakness, numbness, vision field loss, speech changes, and balance problems.
- Persistent, unexplained nausea or vomiting with headache or neuro signs.
Subtle but progressive cognitive/personality change affecting daily function.
Timeline:
- Seek same-day care for seizures, acute neurological deficits, or rapidly worsening headaches.
- Book a clinician visit within one to two weeks for persistent, new, or changing symptoms.
- If symptoms persist beyond two weeks, consult a doctor online with Apollo 24|7 for further evaluation or to arrange
appropriate imaging or referral.
Getting Checked: Diagnosis and Tests That Help
- Clinical exam: A neurological exam assesses strength, reflexes, coordination, sensation, eye movements, and visual fields. An eye doctor may look for papilledema (optic disc swelling), signifying raised intracranial pressure.
- MRI: Preferred for detecting brain tumors and defining location/extent; contrast-enhanced MRI improves detail.
- CT: Useful in emergencies, to detect bleeding or large masses quickly, or when MRI is contraindicated.
- Labs: Endocrine panels if a pituitary tumor is suspected (prolactin, TSH, cortisol, sex hormones). Apollo 24|7 offers home collection for these tests to make the work-up easier.
- EEG: If seizures occurred, to characterize seizure type and guide anti-seizure medication.
- Biopsy: When imaging strongly suggests a tumor, a biopsy (surgical or stereotactic) confirms the diagnosis and tumor
type.
Who’s at Risk? Context Without Alarm
- Age: Some tumors are more common in children (e.g., medulloblastoma) vs. adults (e.g., meningioma, glioma). Most
adult brain tumors are benign meningiomas; malignant gliomas are less common but more serious. - Prior radiation exposure: Increases risk.
- Genetic syndromes: Neurofibromatosis, Li-Fraumeni, and others raise risk.
- Sex and hormones: Meningiomas are more common in women; hormonal factors may play a role.
- Lifestyle: There is no strong evidence that typical mobile phone use causes brain tumors; large studies have not
demonstrated a consistent association.
Perspective: The Lifetime risk of developing a primary malignant brain tumor is relatively low, and most headaches or dizzy spells are not tumors. The key is pattern recognition and timely evaluation when red flags appear.
What Else Could It Be? Common Look-Alikes
- Headaches: Migraines, tension headaches, cluster headaches. Red flags include SNOOP-like features (Systemic
symptoms, Neurologic deficits, Onset sudden, Older age at onset, Pattern change). - Dizziness/balance: Benign paroxysmal positional vertigo (BPPV), vestibular neuritis, medication side effects.
- Vision/hearing: Cataracts, glaucoma, age-related changes, ear wax impaction, otitis media, Meniere’s disease.
- Cognitive/personality: Stress, depression, anxiety, ADHD, sleep deprivation, thyroid disorders, vitamin B12 deficiency.
- Nausea: GI infections, reflux, pregnancy, and medication side effects.
- Hormonal: Thyroid disease, PCOS, menopause/perimenopause.
What can you do Today?: Practical Steps
- Keep a 14-day symptom log: Note time, triggers, intensity (0–10), associated symptoms (vision, weakness, speech), and
impact on daily life. - Vision check: Test peripheral vision at home with a partner (simple finger wiggle test in each quadrant) as a screening;
abnormal results need professional evaluation. - Safety basics: Learn seizure first aid; avoid driving until cleared if you’ve had a seizure or episodes of loss of awareness.
- Medication and history list: Prepare a list for your doctor—current meds, supplements, past head injuries, family
history. - Telehealth triage: Use Apollo 24|7 to discuss patterns, get advice on imaging, or organize labs with home collection
when endocrine clues are present.
Living With Uncertainty: Coping and Support
It’s normal to feel anxious while investigating neurological symptoms. Evidence suggests that having a plan lowers
anxiety—book an appointment, keep your log, and set a check-in date. Consider:
- Support: Talk with a trusted friend or counselor; anxiety and depression can mimic or worsen cognitive symptoms.
- Sleep: Prioritize 7–9 hours; poor sleep can amplify headaches and cognition issues.
- Movement: Gentle activity (walking, yoga) reduces stress and improves blood flow.
- Information hygiene: Stick to trusted sources and avoid doom-scrolling. ABTA, NCI, and NHS pages are reliable.
Prevention Myths and Realities
- Myth: Mobile phones cause brain tumors. Current evidence does not show a clear causal link between typical phone use
and brain tumors.
Reality: You can reduce overall cancer risk with lifestyle basics—don’t smoke, maintain a healthy weight, be active, manage blood pressure and diabetes, and wear helmets to prevent traumatic brain injury.
- Myth: All brain tumors are cancer. Many are benign (e.g., meningioma) but can still cause symptoms by pressing on brain tissue.
Reality: Early evaluation improves outcomes by enabling timely treatment or ruling out serious causes.
Conclusion
Silent does not mean invisible. The brain often signals trouble through small changes in how you think, move, see, or feel. By learning the eight silent signs of a brain tumor and noticing patterns—especially new, persistent, or paired symptoms—you can take smart, timely action without panic. Remember that most similar symptoms have non-tumor causes, but a simple plan makes all the difference: keep a brief symptom log, note red flags like first-time seizures or progressive focal deficits, and book an evaluation if symptoms persist beyond two weeks. Imaging like MRI, eye exams for pressure signs, and targeted hormone tests when pituitary clues are present can clarify the picture quickly. If you need guidance now, consult a doctor online with Apollo 24|7 to discuss your symptoms and next steps; they can also arrange convenient home collections for relevant labs. Your goal isn’t to become a neurologist—it’s to be an informed partner in your own care. When in doubt, ask. When patterns persist, act. That’s how you turn uncertainty into peace of mind.
Consult a Top General Physician
Consult a Top General Physician

Dr. Ajay K Sinha
General Physician/ Internal Medicine Specialist
30 Years • MD, Internal Medicine
Delhi
Apollo Hospitals Indraprastha, Delhi
(225+ Patients)

Dr. Vivek D
General Physician
4 Years • MBBS
Bengaluru
PRESTIGE SHANTHINIKETAN - SOCIETY CLINIC, Bengaluru

Dr. Harshendra Jaiswal
General Physician/ Internal Medicine Specialist
12 Years • MBBS , MD (General medicine)
Kolkata
108 DHANA DHANVANTARI Clinic, Kolkata
(25+ Patients)

Dr. Smitha Nagaraj
General Physician/ Internal Medicine Specialist
15 Years • MBBS, Diploma in Family Medicine
Bengaluru
Apollo Medical Center, Marathahalli, Bengaluru

Dr. Divyashree K
General Physician/ Internal Medicine Specialist
5 Years • MBBS
Bengaluru
Apollo Clinic, JP nagar, Bengaluru
Consult a Top General Physician
Dr. Ajay K Sinha
General Physician/ Internal Medicine Specialist
30 Years • MD, Internal Medicine
Delhi
Apollo Hospitals Indraprastha, Delhi
(225+ Patients)
Dr. Vivek D
General Physician
4 Years • MBBS
Bengaluru
PRESTIGE SHANTHINIKETAN - SOCIETY CLINIC, Bengaluru
Dr. Harshendra Jaiswal
General Physician/ Internal Medicine Specialist
12 Years • MBBS , MD (General medicine)
Kolkata
108 DHANA DHANVANTARI Clinic, Kolkata
(25+ Patients)
Dr. Smitha Nagaraj
General Physician/ Internal Medicine Specialist
15 Years • MBBS, Diploma in Family Medicine
Bengaluru
Apollo Medical Center, Marathahalli, Bengaluru
Dr. Divyashree K
General Physician/ Internal Medicine Specialist
5 Years • MBBS
Bengaluru
Apollo Clinic, JP nagar, Bengaluru
More articles from Brain Tumor



Frequently Asked Questions
1) Are headaches alone a sign of a brain tumor?
Most headaches aren’t due to tumors. Headache red flags include new or progressive headaches, morning-worse pain, or headaches with nausea, vision changes, weakness, or seizures. If headaches persist beyond two weeks, consult a doctor online with Apollo 24|7.
2) What is the early sign of a brain tumor in adults that’s often missed?
Subtle personality or cognitive changes (irritability, focus problems) and vision changes (loss of side vision) are commonly overlooked as early signs of a brain tumor.
3) Is MRI better than CT for detecting a brain tumor?
MRI is generally more sensitive for brain tumors; CT is used in emergencies or when MRI isn’t possible. Ask your clinician which is appropriate for your situation.
4) Can pituitary tumors cause symptoms without headaches?
Yes. Pituitary tumors often present with hormonal symptoms—irregular periods, galactorrhea, low libido, or thyroid-like symptoms—before pain. Apollo 24|7 offers home collection for hormone tests if indicated.
5) When should I see a neurologist for headaches or dizziness?
If symptoms are new and progressive, paired with focal signs (weakness, speech changes, vision loss), or if you’ve had a first-time seizure, seek prompt specialist evaluation.