
What Leads to Signs of Gastritis? Causes & Fixes
Learn the causes, symptoms, triggers, and treatment options for gastritis. Discover diet, lifestyle, and medical strategies to manage and prevent gastritis effectively.

Written by Dr. Dhankecha Mayank Dineshbhai
Reviewed by Dr. Md Yusuf Shareef MBBS, Advanced Certificate Course in Dermatology
Last updated on 13th Jan, 2026

Introduction
If a burning, gnawing pain or bloating in your upper abdomen has you wondering what’s going on, gastritis may be the culprit. Gastritis means inflammation of the stomach lining, and it can be short-lived (acute) or long-standing (chronic). While the symptoms can overlap with indigestion, ulcers, or acid reflux, understanding what leads to signs of gastritis helps you decide what to change at home and when to see a doctor. In this guide, we’ll break down how gastritis starts, the most common causes, and the specific triggers that can set off a flare. You’ll learn how to recognise the signs, how doctors diagnose it, and the treatment options that actually work. We’ll also cover practical diet tips, real-world examples, and what to do if symptoms don’t settle. If symptoms persist beyond two weeks or you notice alarm signs like vomiting blood or black stools, consult a doctor online with Apollo 24|7 for further evaluation.
Gastritis 101: What it is and why it happens
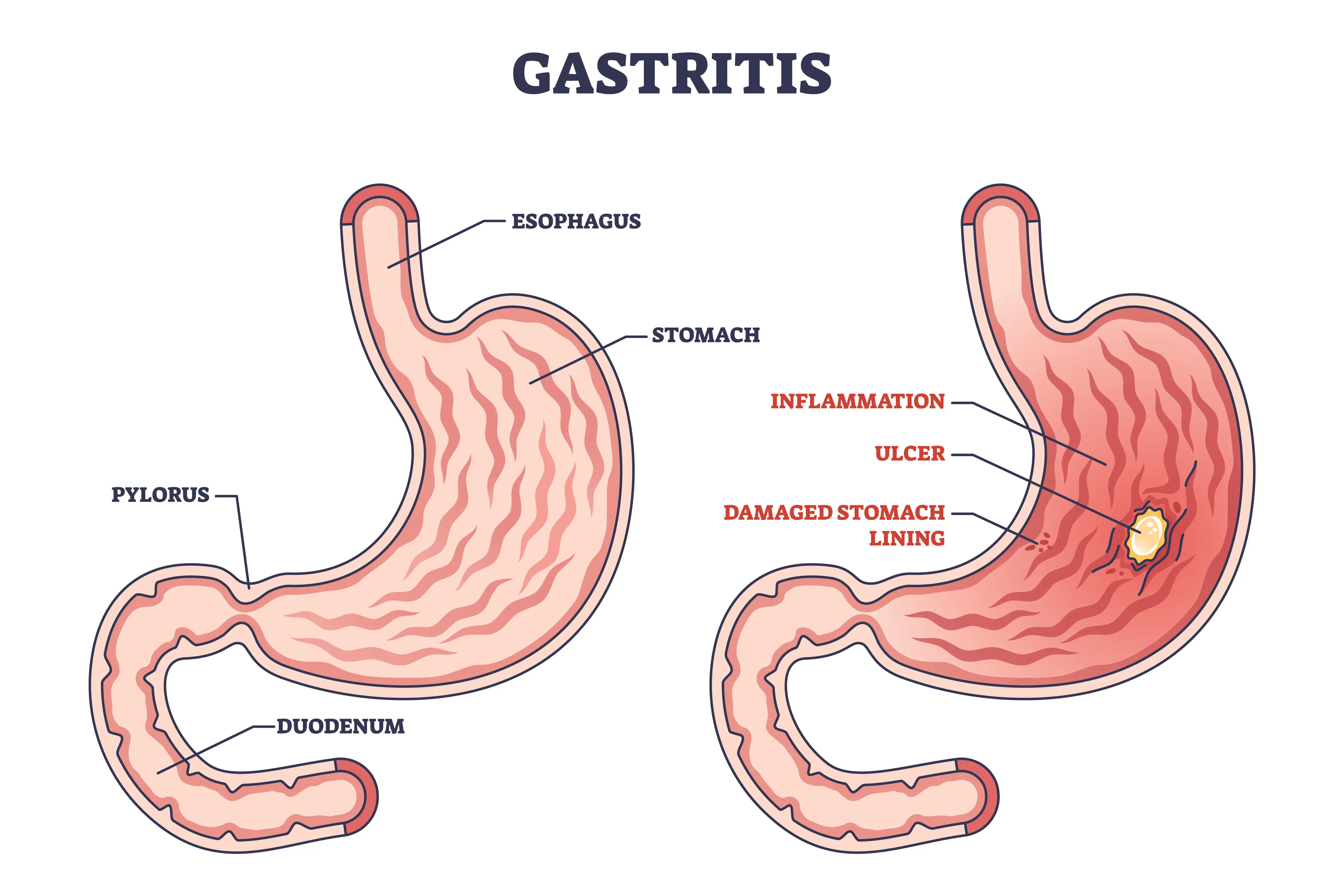
Gastritis is inflammation of the gastric mucosa—the protective lining of your stomach. In a healthy stomach, a thick mucus layer, bicarbonate, and a constant blood supply protect the lining from strong acid and enzymes that help digest food. Gastritis happens when that balance tips: either the defences weaken or the irritants intensify.
Acute gastritis develops suddenly, often due to infections, alcohol, or certain medications like NSAIDs (non-steroidal anti-inflammatory drugs). Chronic gastritis evolves over time, often from persistent Helicobacter pylori infection, autoimmune attack on stomach cells, or repeated irritation. These patterns matter because they influence symptoms, risks like ulcers or anaemia, and the best treatment strategy.
Symptoms do not always match the degree of inflammation. Some people with severe inflammation feel little, while others with mild inflammation have intense discomfort. Persistent or concerning symptoms warrant testing.
Acute vs. chronic gastritis
Acute gastritis often presents with sudden upper abdominal pain, nausea, or vomiting after a triggering event, such as taking high-dose ibuprofen on an empty stomach or heavy alcohol use. Chronic gastritis creeps in, sometimes showing up as vague indigestion, early fullness, or iron/B12 deficiency anaemia without classic pain.
How the stomach lining protects itself
Your stomach secretes mucus and bicarbonate to buffer acid and sheds old cells quickly to heal micro-damage. Prostaglandins help maintain this protection. NSAIDs block prostaglandin production, and H. pylori weakens the mucus layer and inflames the tissue, making the lining easier to injure.
Consult Top Specialists
What leads to signs of gastritis: Root causes and mechanisms
Here's a breakdown of the main causes:
H. pylori infection
Helicobacter pylori is a spiral-shaped bacterium that colonises the stomach lining. It is a leading cause of chronic gastritis and peptic ulcers. H. pylori produces enzymes and toxins that thin the protective mucus and trigger an immune response, resulting in inflammation. Untreated infection can lead to ulcers, atrophy of the stomach lining, and in some cases, increased risk of gastric cancer.
NSAIDs and painkillers
Drugs like ibuprofen, naproxen, diclofenac, and aspirin reduce prostaglandins that protect the stomach lining, making it more vulnerable to acid. Risk increases with higher doses, longer use, older age, prior ulcers, blood thinners, steroids, and alcohol use. Even “as-needed” use on an empty stomach can irritate.
Alcohol, smoking, and bile reflux
Heavy alcohol intake irritates and erodes the stomach lining, causing acute gastritis that can bleed. Smoking reduces blood flow and delays healing. Bile reflux, which occurs when bile backs up from the small intestine into the stomach, can also inflame the lining and mimic acid reflux.
Autoimmune gastritis and vitamin B12
In autoimmune gastritis, the immune system targets parietal cells (acid-producing cells) and intrinsic factor (needed for vitamin B12 absorption). Over time, this can lead to low stomach acid, iron deficiency, and pernicious anaemia due to B12 deficiency. It often goes unnoticed until anaemia or neurological symptoms develop.
Triggers and risk factors you can manage
Here's what can amplify symptoms:
Diet patterns and specific foods
Large, late-night meals, high-fat fried foods, highly acidic or very spicy dishes, and caffeine can worsen pain or reflux in some people. Smaller, balanced meals with lean protein, cooked vegetables, whole grains, and limited irritants often feel better. Fermented dairy or yoghurt may be soothing for some, but dairy triggers reflux in others.
Stress, sleep, and the gut-brain axis
Everyday stress can sensitise the gut, speed up or slow down motility, and heighten pain perception. Severe physiological stress can cause stress-related erosive gastritis due to poor blood flow and increased acid. Poor sleep timing and late meals can also increase nocturnal acid exposure.
Age, genetics, and comorbidities
Older adults have thinner mucosa, take more medications, and are more likely to have H. pylori or autoimmune gastritis. Conditions like liver disease, kidney disease, or diabetes can alter stomach function and healing. Family history may raise risk for autoimmune gastritis.
What gastritis feels like: Signs, symptoms, and red flags
Here's how gastritis typically presents:
Typical symptoms
Common signs of gastritis include:
- Burning or gnawing pain in the upper abdomen, often after eating
- Bloating, belching, or early fullness
- Nausea or vomiting
- Loss of appetite
- Indigestion-like discomfort
Alarm features that need urgent care
Seek immediate care for:
- Vomiting blood or coffee-ground material
- Black, tarry stools (melena)
- Unintentional weight loss
- Persistent vomiting or trouble swallowing
- Severe or worsening pain, especially with fainting or chest pain
Pain location and timing can help identify the type of gastritis. Pain right after meals suggests antral gastritis or ulcers; pain a few hours after eating may indicate a duodenal ulcer; nighttime awakening often points to acid-peptic activity.
How doctors diagnose gastritis
Here's how diagnosis is typically made:
H. pylori testing (breath, stool, biopsy)
Noninvasive tests include the urea breath test and stool antigen test. Both are highly accurate but require stopping PPIs and antibiotics beforehand to avoid false negatives. A biopsy during endoscopy is another option.
Endoscopy and biopsy
Upper endoscopy lets a clinician visualise the stomach lining, detect erosions or ulcers, and take biopsies to confirm gastritis type. It is recommended if you have alarm features, are older with new symptoms, or do not improve with initial therapy.
Labs and imaging
A complete blood count checks for anaemia; iron studies and vitamin B12 may reveal chronic blood loss or autoimmune gastritis. Occult blood testing may be used if bleeding is suspected. Imaging is rarely needed unless complications or other diagnoses are suspected.
Treatment that works: From quick relief to root-cause fixes
Here's what works for managing gastritis:
Acid suppression (PPIs, H2 blockers, antacids)
Proton pump inhibitors like omeprazole, pantoprazole, or esomeprazole are strongest for healing inflammation and ulcers. H2 blockers such as famotidine are helpful for milder symptoms or night-time acid. Antacids provide quick, short-lived relief. Take PPIs 30–60 minutes before meals for best effect. Avoid long-term use without medical guidance.
H. pylori eradication therapy
If H. pylori is confirmed, combination antibiotics plus a PPI for 10–14 days are required. Confirm eradication 4+ weeks after therapy using a breath or stool test.
Medication stewardship (NSAIDs, aspirin)
If NSAIDs triggered your symptoms, stop them if possible. If you must continue, use the lowest effective dose for the shortest time, consider switching to COX-2 selective agents, or add a PPI to protect the stomach. Never stop prescribed aspirin without medical advice.
Probiotics and adjuncts
Probiotics can improve H. pylori eradication rates and reduce antibiotic side effects. Alginate-based formulations may reduce reflux, and sucralfate can protect irritated mucosa. Herbs like deglycyrrhizinated licorice may be used, but evidence is limited. Always discuss supplements with a clinician.
Eating and living well with gastritis
Here's how to adjust diet and daily habits:
A 2–4-week flare-calming meal plan
- Small, frequent meals every 3–4 hours
- Easy-to-digest protein such as eggs, fish, tofu, and yoghurt if tolerated
- Cooked vegetables and low-acid fruits like bananas and melons
- Whole grains like oatmeal or rice
- Healthy fats in modest amounts
- Hydration with water or herbal teas such as ginger or chamomile
What to limit vs. what to avoid
Identify personal triggers with a simple journal. Avoid smoking and minimise alcohol, especially during a flare.
Daily routine hacks that make a difference
- Do not lie down within 2–3 hours after dinner
- Elevate the head of your bed if nighttime symptoms persist
- Target 7–8 hours of sleep; keep meal timing regular
- Practice brief stress-reduction exercises
- Keep NSAIDs to a minimum; never on an empty stomach
Complications, prevention, and myths to avoid
Here's what to know:
Ulcers, bleeding, and anaemia
Unchecked gastritis can progress to ulcers and bleeding. Chronic inflammation may lead to iron deficiency anaemia, while autoimmune gastritis can cause vitamin B12 deficiency. Early diagnosis and treatment prevent most complications.
Cancer risk and surveillance
Chronic H. pylori gastritis increases the risk for gastric cancer. Eradicating H. pylori reduces this risk. People with advanced atrophic gastritis or intestinal metaplasia may require surveillance endoscopy.
Common myths
- Spicy foods trigger symptoms but do not typically cause inflammation.
- Milk may soothe briefly, but the fat/protein can stimulate acid later.
- Apple cider vinegar may aggravate symptoms and harm the lining.
Special situations: Pregnancy, older adults, athletes
Here's how management may differ:
Medication safety
In pregnancy, focus on non-drug measures first. Antacids and some H2 blockers may be used; PPIs are considered when needed under medical guidance. Older adults are more sensitive to NSAIDs and polypharmacy.
Nutrition, B12, and iron
Older adults and those with autoimmune gastritis should periodically check iron and vitamin B12. Athletes using frequent NSAIDs should consider protective strategies to minimise gut irritation.
Conclusion
Gastritis is a pattern of inflammation with multiple potential causes, each requiring a tailored approach. Acid suppression can quickly ease pain, but lasting relief comes from addressing the driver: eradicating H. pylori, adjusting NSAID use, reducing alcohol and smoking, or treating autoimmune gastritis. Layer in smart lifestyle choices—smaller meals, earlier dinners, adequate sleep—and most people improve within weeks. Keep an eye on alarm symptoms. If symptoms persist beyond two weeks, consult a doctor online with Apollo 24|7 for guidance and testing.
Consult Top Specialists
Consult Top Specialists

Dr Rohit Sureka
Gastroenterology/gi Medicine Specialist
15 Years • MBBS, DNB General Medicine, DNB Gastroenterology
Jaipur
Apollo 247 virtual - Rajasthan, Jaipur

Dr. Shivaraj Afzalpurkar
Gastroenterology/gi Medicine Specialist
13 Years • MBBS, MD General medicine (Gold medalist), DrNB (Gastroenterology), MNAMS
Bengaluru
Apollo Clinic, JP nagar, Bengaluru

Dr Piyush Vishwakarma
Gastroenterology/gi Medicine Specialist
11 Years • MBBS, MD, DrNB,
Delhi
Apollo Hospitals Indraprastha, Delhi
(25+ Patients)

Dr. Amit Pandita
Gastroenterology/gi Medicine Specialist
10 Years • MBBS. MD (INTERNAL MEDICINE) DrNB (GASTROENTEROLOGY AND HEPATOLOGY)
Delhi
Apollo Hospitals Indraprastha, Delhi

Dr Abhishek Tiwari
Minimal Access/Surgical Gastroenterology
15 Years • MBBS, MS, Diabetic Foot Course (Pisa, Italy)
Delhi
Apollo Hospitals Indraprastha, Delhi
Consult Top Specialists
Dr Rohit Sureka
Gastroenterology/gi Medicine Specialist
15 Years • MBBS, DNB General Medicine, DNB Gastroenterology
Jaipur
Apollo 247 virtual - Rajasthan, Jaipur
Dr. Shivaraj Afzalpurkar
Gastroenterology/gi Medicine Specialist
13 Years • MBBS, MD General medicine (Gold medalist), DrNB (Gastroenterology), MNAMS
Bengaluru
Apollo Clinic, JP nagar, Bengaluru
Dr Piyush Vishwakarma
Gastroenterology/gi Medicine Specialist
11 Years • MBBS, MD, DrNB,
Delhi
Apollo Hospitals Indraprastha, Delhi
(25+ Patients)
Dr. Amit Pandita
Gastroenterology/gi Medicine Specialist
10 Years • MBBS. MD (INTERNAL MEDICINE) DrNB (GASTROENTEROLOGY AND HEPATOLOGY)
Delhi
Apollo Hospitals Indraprastha, Delhi
Dr Abhishek Tiwari
Minimal Access/Surgical Gastroenterology
15 Years • MBBS, MS, Diabetic Foot Course (Pisa, Italy)
Delhi
Apollo Hospitals Indraprastha, Delhi
More articles from Gastritis


Frequently Asked Questions
How do I know if it’s gastritis or just indigestion?
Gastritis often brings burning upper abdominal pain, nausea, and early fullness. If symptoms persist more than two weeks or include alarm signs, get evaluated and ask about H. pylori testing.
Can H. pylori spread to family members?
Yes. H. pylori can spread via saliva and close contact. Symptomatic household members should discuss testing with their provider.
What foods should I avoid during a gastritis flare?
Temporarily limit alcohol, large/fatty meals, very spicy or acidic foods, and excessive coffee. Focus on small, frequent meals with lean proteins and cooked vegetables.
How long does it take gastritis to heal?
Many cases improve within 2–4 weeks with acid suppression and lifestyle changes. Chronic or autoimmune gastritis may require ongoing management.
Is it safe to keep taking ibuprofen if I have gastritis?
Frequent NSAID use can worsen gastritis. Discuss alternatives, dose minimisation, or protective therapy with your clinician. Never stop prescribed aspirin for heart protection without medical advice.