
Guide to Planning Baby 40: What You Need to Know
Guide to plan a baby after 40, why it is different, myths, facts, know about fertility, safe practices for pregnancy, lifestyle upgrades and more.


Introduction
Thinking about planning a baby at 40 or beyond? You’re not alone. More people are choosing to start or grow their families later, thanks to longer life expectancy, evolving careers, and personal goals. While getting pregnant after 40 can be absolutely possible, it’s also different from conceiving in your 20s or early 30s. Fertility declines, certain pregnancy risks rise, and choices about testing and treatment may feel more complex. The good news: with a smart preconception plan, evidence-based care, and the right support, you can improve your odds of a healthy pregnancy and baby.
This guide brings together what the top medical sources say about fertility in your 40s—plus practical steps for preconception, lifestyle upgrades, timing, assisted options (like IVF and donor eggs), pregnancy screening, and postpartum care. If you’re trying to conceive at 40, or supporting a partner who is, here’s what you need to know to make confident choices for your body, your baby, and your life.
Consult a Top Gynaecologist for Personalised Advice
Why planning a baby at 40 is different
The reasons behind it include:
Age-related fertility changes in plain language
Fertility naturally declines with age because both the number of eggs (quantity) and their genetic integrity (quality) decrease over time. By 40, your chance of conception per cycle is typically around 5% compared with about 20–25% per cycle in your 20s. The main change is egg quality: more eggs carry chromosomal errors that can reduce fertilisation chances, raise miscarriage rates, or lead to chromosomal conditions. Miscarriage risk also rises with age; at 40, estimates approach 40%, and are higher after 43, though exact figures vary across studies and populations.
Myths vs facts about getting pregnant at 40
- Myth: “A high AMH means I’ll get pregnant quickly.” Fact: AMH predicts ovarian response to stimulation (e.g., IVF), not your exact chance of natural pregnancy next month.
- Myth: “It’s impossible to conceive naturally at 40.” Fact: Many do conceive naturally, especially with regular cycles and timed intercourse—though odds are lower and timelines can be longer.
- Myth: “If I’m healthy and fit, age won’t matter.” Fact: Health helps, but age still independently impacts egg quality and risks like gestational diabetes [5].
Know your fertility: odds, markers, and myths
The fertility features include:
Egg quality vs quantity: what actually matters
Quantity refers to how many eggs are left (ovarian reserve). Quality refers to the genetic health of eggs—critical for an embryo to develop into a healthy baby. As age increases, egg quality drops faster than quantity, which explains why time-to-pregnancy lengthens and miscarriage risk rises even when cycles appear regular [2][4]. For many at 40+, egg quality is the main bottleneck.
AMH, FSH, and AFC: useful, but not crystal balls
- AMH (anti-Müllerian hormone): reflects ovarian reserve. Low AMH suggests fewer eggs for IVF retrieval but does not reliably predict how long it will take to conceive naturally [4].
- FSH (follicle-stimulating hormone), day 3: can rise as the brain works harder to mature follicles, but single values fluctuate.
- AFC (antral follicle count): ultrasound count of small follicles. Like AMH, it helps anticipate IVF response.
How long to try before getting help at 40+
If you’re 40 or older, many experts recommend seeking a fertility evaluation after 3–6 months of trying—or even promptly if you prefer a proactive check, especially with irregular cycles or known conditions. If you’ve been trying without success, or cycles are erratic, consult a fertility specialist. If you’re in India, you can consult a doctor online with Apollo24|7 to discuss evaluation options and next steps.
Preconception checkup, labs, and supplements
Medical review, medications, and vaccines
A preconception visit ensures your body is ready for a baby. Your clinician will review your history (blood pressure, diabetes, thyroid disease, PCOS), medications (e.g., some acne or blood pressure drugs need switching), and vaccinations. Ideally, update:
- MMR and varicella before pregnancy if not immune
- Influenza (any trimester) and Tdap (27–36 weeks) during pregnancy
- COVID-19 as recommended
Key labs and what they tell you
Common pre-pregnancy labs include CBC (anaemia), TSH (thyroid), HbA1c or fasting glucose (diabetes risk), rubella/varicella immunity, and STI screening. Consider vitamin D, ferritin, and lipid panel as part of general health. If you’re in India, Apollo24|7 offers convenient home collection for tests like vitamin D, thyroid profile, and HbA1c.
Folic acid, prenatal vitamins, and optional supplements
- Start folic acid 400–800 mcg daily (or 4 mg if prior neural tube defect—ask your clinician) at least 1 month before conception.
- Prenatal vitamin: typically includes iodine, iron, B12, and DHA/EPA (can be separate).
- Consider CoQ10 (ubiquinol) after discussing with your doctor; small studies suggest potential benefits for egg quality, but evidence is not definitive. Avoid high-dose vitamin A and any supplement not reviewed with your clinician.
Lifestyle upgrades that move the needle
These include:
Weight, movement, and sleep basics
Aim for a healthy BMI before pregnancy; both higher and very low BMI can affect fertility and pregnancy outcomes [5]. Build a routine with:
- 150 minutes of moderate aerobic activity weekly, plus strength training (2 days/week)
Pelvic floor activation and core stability work - 7–9 hours of sleep nightly; prioritise consistent sleep-wake times
Smart nutrition, caffeine, and alcohol limits
- Pattern: a Mediterranean-style diet (vegetables, fruits, legumes, whole grains, fish, olive oil) supports overall fertility and pregnancy health.
- Protein: include lean proteins; omega-3s (fatty fish like salmon) twice weekly.
- Caffeine: limit to ≤200 mg/day when trying to conceive and in pregnancy (about one 12-oz coffee).
- Alcohol: if you’re actively trying and could conceive, consider minimising or avoiding in the luteal phase; avoid once pregnant.
Mastering timing: ovulation tracking at 40+
OPKs, cervical mucus, and apps
At 40, cycle variability can increase. Use multiple methods:
- Ovulation predictor kits (OPKs): detect LH surge; intercourse the day of the surge and the next day is reasonable.
- Cervical mucus: creamy to clear/stretchy indicates fertile window.
- Apps: helpful for logging, but don’t rely on predictions alone; your cycle may shift month-to-month.
- Mid-luteal progesterone blood test can confirm ovulation if cycles are unclear.
Perimenopause cycles and timing intercourse
- Perimenopause can mean shorter follicular phases and occasional anovulatory cycles. Practical tips:
- Start OPKs a few days earlier than you used to; consider testing twice daily around your typical surge days.
- Aim for intercourse every 1–2 days during the fertile window for the best chances.
- If cycles are <21 days, >35 days, or widely variable, discuss evaluation—especially at 40+.
Your options: natural conception vs assisted paths
IUI, IVF, ICSI—what they are and when to consider them
- IUI (intrauterine insemination): places washed sperm into the uterus around ovulation. Success at 40 is modest per cycle, improves if specific issues are addressed (e.g., mild male factor).
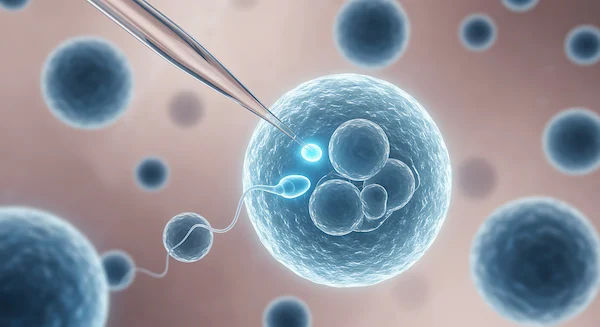
- IVF (in vitro fertilisation): retrieves eggs, fertilises them in the lab, and transfers embryos. With your own eggs at 40, per-cycle live birth rates are commonly around 15–20%, declining sharply after 42; results vary by clinic and individual factors.
- ICSI: injects a single sperm into an egg, used mainly for male factor or prior fertilisation issues.
Donor eggs, embryos, and adoption—success and trade-offs
- Donor eggs: success rates largely reflect donor age; per transfer, live birth can exceed 40–50% in many programs [8].
- Donor embryos: often more affordable than fresh donor cycles; success depends on embryo quality and lab standards.
- Adoption: a meaningful path to parenthood; timelines and costs vary.
- Unique insight: Ask clinics for cumulative live-birth rates per number of transfers, not just “per cycle.” That gives a clearer picture of your overall odds over 1–3 attempts.
If you’ve been trying at 40+ with no success, or your condition does not improve after trying these methods, book a consultation with a fertility specialist. In India, you can consult a doctor online with Apollo24|7 for guidance tailored to your situation.
Safer pregnancy after 40: risks and prevention
Gestational diabetes, hypertension, and preeclampsia
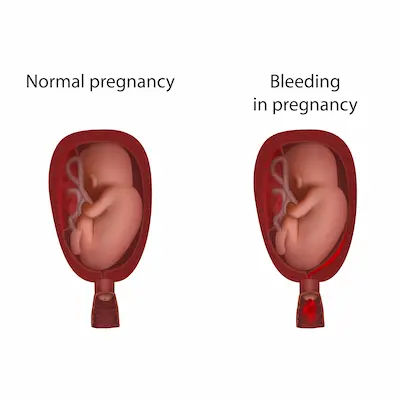
Pregnancy at 40+ carries higher risks of gestational diabetes, high blood pressure, preeclampsia, placenta previa, and cesarean delivery. Early identification and control of risk factors can help. If you have a history of hypertension, diabetes, kidney disease, or autoimmune conditions, optimisation before pregnancy is critical.
Low-dose aspirin and early screening—who benefits
Low-dose aspirin (81 mg) starting between 12–16 weeks can reduce preeclampsia risk in higher-risk pregnancies. It’s recommended for those with high-risk factors and for some with multiple moderate-risk factors; maternal age >35 is a moderate risk factor, but not the sole basis for aspirin—discuss your personal risk profile with your clinician [6]. Consider earlier screening for diabetes if you have risk factors (e.g., elevated BMI, prior GDM, family history). Lifestyle measures—nutrient-dense diet, movement, adequate sleep—also reduce risk.
Smart prenatal care and screening
NIPT, NT, CVS, and amnio—choosing what’s right
- NIPT (noninvasive prenatal testing) from ~10 weeks screens for common chromosomal conditions with high sensitivity/specificity; positive screens should be confirmed with diagnostic testing.
- NT scan (11–14 weeks) measures nuchal translucency; often combined with blood tests.
- CVS (10–13 weeks) and amniocentesis (15–20 weeks) provide diagnostic certainty but have small procedure-related risks.
- At 40, the baseline chance of chromosomal conditions is higher, which changes screening test performance and counselling. Work with a genetic counsellor to choose tests aligned with your values.
Ultrasound milestones, growth monitoring, and induction
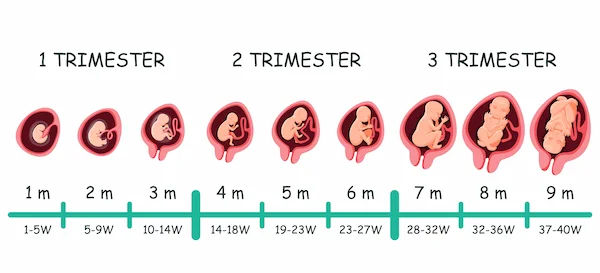
- Dating scan: around 8–10 weeks
- Anatomy scan: 18–22 weeks
- Growth scans: often added in the third trimester at 40+ to monitor placental function and fetal growth
- Some providers discuss induction near term (e.g., by 39–40 weeks) to balance rising stillbirth risk with induction-related risks; decisions are individualised.
Stress science, relationships, and your support circle
Trying to conceive at 40 can be emotionally intense. Chronic stress can disrupt sleep, appetite, and coping—even if it doesn’t directly block ovulation. Protect mental health with:
- Regular therapy or support groups
- Mindfulness/relaxation practices (10–15 minutes daily)
- Scheduled “non-baby” conversations and date time
- Sharing roles and expectations with your partner or support person
Birth, postpartum, and newborn care essentials
Delivery options and recovery realities
Cesarean rates are higher at 40+, but many have vaginal births. Discuss:
- Induction reasons/timing
- VBAC eligibility if you’ve had a prior cesarean
- Pain relief preferences (epidural vs non-pharmacologic)
- Recovery may take longer; prioritise rest, nutrition, hydration, and help at home. Pelvic floor physiotherapy can support healing and continence.
Feeding, pelvic floor, and the 4th trimester plan
Feeding your baby (breast, formula, or combo) is personal—get lactation support early if needed. Line up:
- A 4th-trimester plan: meals, help, sleep shifts
- Postpartum visit dates (including 1–2 weeks if you have mood concerns)
- Paediatrician selection and newborn care basics (safe sleep, car seat)
When to seek help and red flags
Trying-to-conceive timelines at 40+
- At 40+: consider a fertility evaluation after 3–6 months of trying (earlier if cycles are irregular or you prefer proactive planning) [4].
- Immediate evaluation if you have risk factors: very irregular cycles, suspected endometriosis, prior pelvic infection or surgery, or known male factor.
- If you’re in India and want a quick start, Apollo24|7 can help you book a virtual consult and order baseline labs with home collection.
Pregnancy warning signs you shouldn’t ignore
Call your clinician urgently for:
- Severe headache, vision changes, sudden swelling (possible preeclampsia)
- Persistent abdominal pain, bleeding, and fluid leakage
- Decreased baby movements after 28 weeks
- Signs of infection or high fever
- If symptoms are severe, seek emergency care.
Conclusion
Planning a baby at 40 is both an act of hope and of strategy. While biology changes the odds, knowledge and preparation meaningfully shift them in your favour. Start with a thorough preconception checkup, folic acid, and lifestyle habits that support fertility. Track ovulation with a layered approach, and set a clear timeline for when to seek help. Understand your full range of options from natural conception to IVF and donor eggs and ask clinics for data that reflect your true chances over time. During pregnancy, choose screening and care pathways that align with your values and medical needs, and stay proactive about risk prevention. Just as important, plan for life around your baby: finances, work leave, emotional support, and postpartum recovery.
Consult a Top Gynaecologist for Personalised Advice
Consult a Top Gynaecologist for Personalised Advice

Dr Arpita
Obstetrician and Gynaecologist
6 Years • MS OBG
Bengaluru
Apollo Medical Center, Marathahalli, Bengaluru

Dr. Millie Dasgupta
Obstetrician and Gynaecologist
10 Years • MBBS,DNB (Obst. & Gynae.)
Kolkata
MCR SUPER SPECIALITY POLY CLINIC & PATHOLOGY, Kolkata

Dr. Barsha Subhadarshine
Obstetrician and Gynaecologist
5 Years • MBBS,MS (Obst. & Gynae.)
Kolkata
VDC Clinic, Kolkata

Dr. Srinka Mukherjee
Obstetrician and Gynaecologist
7 Years • MBBS, MS Obstetrics & Gynaecology
Kolkata
VDC Clinic, Kolkata

Dr. Biplab Mukhopadhay
Obstetrician and Gynaecologist
14 Years • MBBS, DNB - Obstetrics & Gynecology, MNAMS, FMAS, Diploma In Minimal Access Surgery
New Delhi
THE CLINICS, New Delhi
Consult a Top Gynaecologist for Personalised Advice
Dr Arpita
Obstetrician and Gynaecologist
6 Years • MS OBG
Bengaluru
Apollo Medical Center, Marathahalli, Bengaluru
Dr. Millie Dasgupta
Obstetrician and Gynaecologist
10 Years • MBBS,DNB (Obst. & Gynae.)
Kolkata
MCR SUPER SPECIALITY POLY CLINIC & PATHOLOGY, Kolkata
Dr. Barsha Subhadarshine
Obstetrician and Gynaecologist
5 Years • MBBS,MS (Obst. & Gynae.)
Kolkata
VDC Clinic, Kolkata
Dr. Srinka Mukherjee
Obstetrician and Gynaecologist
7 Years • MBBS, MS Obstetrics & Gynaecology
Kolkata
VDC Clinic, Kolkata
Dr. Biplab Mukhopadhay
Obstetrician and Gynaecologist
14 Years • MBBS, DNB - Obstetrics & Gynecology, MNAMS, FMAS, Diploma In Minimal Access Surgery
New Delhi
THE CLINICS, New Delhi
More articles from pregnancy


Frequently Asked Questions
How long should I try before seeing a fertility specialist at 40?
Many experts advise evaluation after 3–6 months of trying to conceive at 40+, or sooner if cycles are irregular or you prefer a proactive plan (trying to conceive at 40 timeline).
What are my chances of getting pregnant at 40 naturally?
On average, per-cycle chances at 40 are around 5% (varies by health and cycle regularity). Many still conceive naturally, particularly with optimised timing and health.
Do I need NIPT if I’m over 40?
ACOG now supports offering NIPT to all pregnant people, regardless of age. At 40, baseline risk is higher, so NIPT can be particularly informative. Positive screens require diagnostic confirmation.
Will low-dose aspirin help me prevent preeclampsia?
It can reduce risk for those with high-risk or multiple moderate-risk factors. Maternal age >35 is a moderate risk factor; discuss your individual profile before starting 81 mg daily.
Are AMH levels a reliable predictor of natural fertility?
AMH reflects ovarian reserve and is useful for IVF planning, but low AMH doesn’t reliably predict reduced natural fertility in the short term. It’s one piece of the puzzle—not a forecast (AMH levels and fertility).